
Covid-19 has reached the community spread phase. Developed or underdeveloped, rich or poor, all countries are affected by this today. However, they are facing these challenges – shortages in medical supplies and difficulty stopping its spread – in different magnitudes. In an attempt to stop the spread to save lives, Prime Minister Narendra Modi announced a 21-day lockdown, starting from 25th of March. Developing countries across the globe are looking down quickly, after witnessing the helplessness of the US, UK and the rest of Europe – though these are the countries with much stronger healthcare systems and much better availability of doctors. In Italy, doctors are forced to prioritize whom to save and whom to leave untreated.
India’s healthcare infrastructure is incapable of dealing with this crisis today. Shortages in medical supplies and an inability to provide adequate testing are the major issues. However, the Prime Minister’s announcement to allocate 15,000 crore rupees (USD 2 billion) for building infrastructure can strengthen the fight against coronavirus. Also, state governments are trying to expand facilities to deal with this situation.
The majority of Indians finance their healthcare themselves. About 62 percent of households’ expenditure on healthcare in 2017 was made through out-of-pocket payments. In comparison, the equivalent figures for the European Union (excluding UK) is 22.29 percent and for the USA and UK it is 11 percent and 16 percent, respectively (Table 1). While many patients diagnosed with Covid-19 will need Intensive Care Unit (ICU), there is no clarity from the government regarding who will pay these expenses.
Table 1: Out-of-pocket health expenditures (% of total)
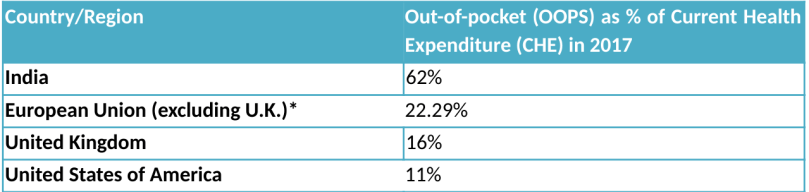
Source: WHO Global Health Expenditure Database.
* EU’s figures is an average of figures of all members’, excluding U.K.
There are lessons to learn from each affected country. For instance, Italy, which ranks second in the world in terms of healthcare performance, has failed to tackle the problem of shortages. One of the reasons behind the collapse of Italy’s healthcare system is that 20-30 percent of its healthcare workers, too, got infected.
In India, there is a major shortage in the availability of beds in the hospitals. Bihar (one of the least-developed states) has 0.12 beds per thousand people, which is the state with the fewest beds per person. The poorest state of India, Odisha, according to Raghuram Rajan commission, has 0.38 beds per thousand people. In the Northeastern part of India, Assam and Manipur has 0.32 and 0.48 beds, respectively, which is below the national average of 1.13 beds per thousand of people. Other states of the Northeast and Southern India have better capacity to serve patients – near to or above the national average (Figure 1 and Figure 2). The states of Bihar, Madhya Pradesh, Rajasthan and Uttar Pradesh (the so-called BIMARU states) , where one in every four persons is below the poverty line, have less capacity than the national average (Figure 3) and more than half of India’s population lives in these (four) states.
Figure 1: Beds available per thousand in the Northeastern States
 Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
Figure 2: Beds available per thousand in the Southern states
 Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
Figure 3: Beds Available per Thousand in the BIMARU States
 Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
Source: Computation using Ministry of Health and Family Welfare and RBI’s population data
In Italy, the number of beds per thousand is 3.4 and in China it is 4.2 (according to the World Bank in 2012). It is only in recent years that India increased its bed capacity from 0.7 beds per thousand, in 2011, to 1.13 today. But still it is insufficient to deal with this crisis. The situation in Europe and North America indicates that it would be a huge challenge for India to fight this pandemic with the current amount of resources to its disposal.
Some countries, like Norway, Germany and South Korea, performed testing at a bigger scale. As of the 20th March, South Korea performed, the highest amount of tests (316664), followed by Italy’s 206886 tests. And, as of the 30th March 2020, only 38442 tests have been performed in India (and India has a population of 1.2 billion people) (Table 2). Pace of testing, in India is very slow and it can certainly encourage the spread. At this point, when numbers of cases are increasing steadily, one viable strategy could be to conduct tests through random sampling. Moreover, there are only 118 government approved laboratories in India which are capable of performing covid-19 tests. Apart from it, obviously, there are private labs, which are now authorized to conduct tests, and companies making self testing kits.
Table 2: Tests performed
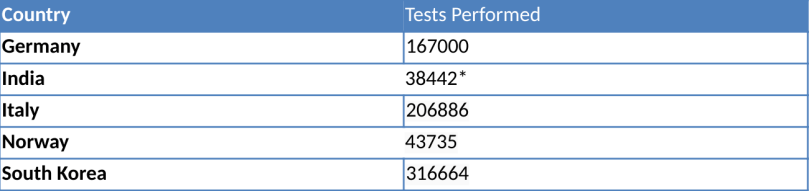
Source: Our World in Data. Available at: https://ourworldindata.org/coronavirus-testing-source-data
* figure is from Live mint’s report, 30th March 2020.
The acute shortages of doctors can result in a deadly chaos if the crisis balloons. Doctors, like in Italy, will be forced to decide whose life is more important. The only solution appears to be to stay at home, which is not easy for the majority of Indians. About 77.9 percent of the workforce in India, is self-employed. The majority of these workers work in the informal sector. There are packages announced by the central government, and almost by every state Government, but the amount of support is still inadequate.
For instance, packages amounting to USD 22.5 billion were announced by the Finance Minister which includes free cereals, cooking gas and other essential goods for the poor. The announcements of cash transfers of Rs 1,000 (USD 13.25) for the people registered under Mahatma Gandhi National Rural Employment Act (MGNREGA) {1} and of Rs 500 (USD 6.62) every month for the next three months to women in their Jan-Dhan Bank accounts {2} have also been made. Overall, the package announced by the central government has wider coverage than the states have provided. Although it can provide some (albeit little) relief to the poor, it does not cover the self employed and small businesses which are, too, suffering due to the lockdown.
Today, the top six affected countries from the virus are USA, Italy, Spain, China, Germany and Iran. All of these countries have a stronger capacity to serve patients than India (Table 3). The announcement of the lockdowns is a bold step, as it will be difficult to bear the economic losses caused by it. The whole global economy is on a ventilator and the aftermath of the pandemic will be difficult to tackle for the entire world. In this context, the weakness of the Indian infrastructure and response so far is even more worrying.
Table 3: Beds per 1000 population

Source: World Bank. Data from World Health Organization. Available at: https://data.worldbank.org/indicator/SH.MED.BEDS.ZS. Figure years: *2012, **2013, and ***2014.
Aru Bhardwaj is an undergraduate student in Economics at Punjabi University, India. He tweets at @AruEcon
Notes:
{1} MGNREGA is an Indian labour law and social security measure, launched in 2006, under which it becomes the responsibility of the Government to provide at least 100 days employment to one person from a rural household. If it fails in providing that then the individual is entitled to an unemployment allowance. Official website: https://nrega.nic.in
{2} The Government of India launched a scheme called Pradhan Mantri Jan-Dhan Yojana (Peoples’ wealth scheme) in 2014, under which every individual is given an opportunity to get a bank account without any restriction of maintaining minimum balance. There are 38.28 crore beneficiaries so far. Official website: https://pmjdy.gov.in/
